Cms 1500 form instructions Greenslopes

HCFA-1500 eDirect Forms HCFA 1500 & UB-04 Claim Form CMS 1500 Billing Instructions Guide Date of Publication: 05/04/2018 The CMS 1500 form, previously known as the HCFA 1500 form, is a billing form maintained by the
CMS 1500 Instructions Address (Geography) Health
Instructions on how to fill out the CMS 1500 Form. Medicaid CMS-1500 Instructions. PDF download: Medicare Claims Processing Manual – CMS. www.cms.gov. 1.0 CMS-1500 Claim Form Instructions. Item # Description., Medicare HMO Billing Instructions for Professional Providers (New CMS-1500 Claim Form) Blocks 11 and 11a through 11c – Enter the information applicable to the.
Instructions on how to fill out the CMS 1500 Form telephone number. Item 6 Patient’s Relationship to Insured If Medicare is primary, leave blank. CMS-1500 (02-12) Claim Form Instructions when Medicare is Secondary. Complete the items below on the CMS-1500 (02-12) claim form or electronic equivalent, in addition
CMS 1500 (02/12) INSTRUCTIONS FOR WAIVER SERVICES You must write “WAIVER” at the top center of the claim form! Locator # Description Instructions Alerts PLEASE PRINT OR TYPE APPROVED OMB-0938-1197 FORM 1500 ut the accident on the claim form; Use the two-digit POS codes specified by CMS.
Fill nucc org 1500 claim form 2012-2018 denise instantly, download blank or editable online. Sign, fax and printable from PC, iPad, tablet or mobile. No software. Try PLEASE PRINT OR TYPE APPROVED OMB-0938-1197 FORM 1500 ut the accident on the claim form; Use the two-digit POS codes specified by CMS.
Providers may use these instructions to complete this form. The CMS-1500 claim form has space for physicians and suppliers to provide information on other health How to Use SimClam™ CMS‐1500 General Instructions for You have the option to print the primary or secondary CMS‐1500 form
CMS 1500 Instructions The following sections must be completed correctly or the bill will be returned and payment may be delayed or rejected. Note: If using the CMS medicare supplemental insurance (PDF download) medicare coverage (PDF download) medicare supplement plans (PDF download) medicare part d (PDF download)
Instructions and guideline for CMS 1500 claim form and UB 04 form. Tips and updates. Detailed review of all the fields and box in CMS 1500 claim form and UB 04 form from the current professional claim form [CMS 1500 (08-05)] to the new professional claim For complete billing instructions for this field refer to the National
Item number Required Field? Description and Instructions. 1 Optional Indicate the type of health insurance for which the claim is being submitted. medicare supplemental insurance (PDF download) medicare coverage (PDF download) medicare supplement plans (PDF download) medicare part d (PDF download)
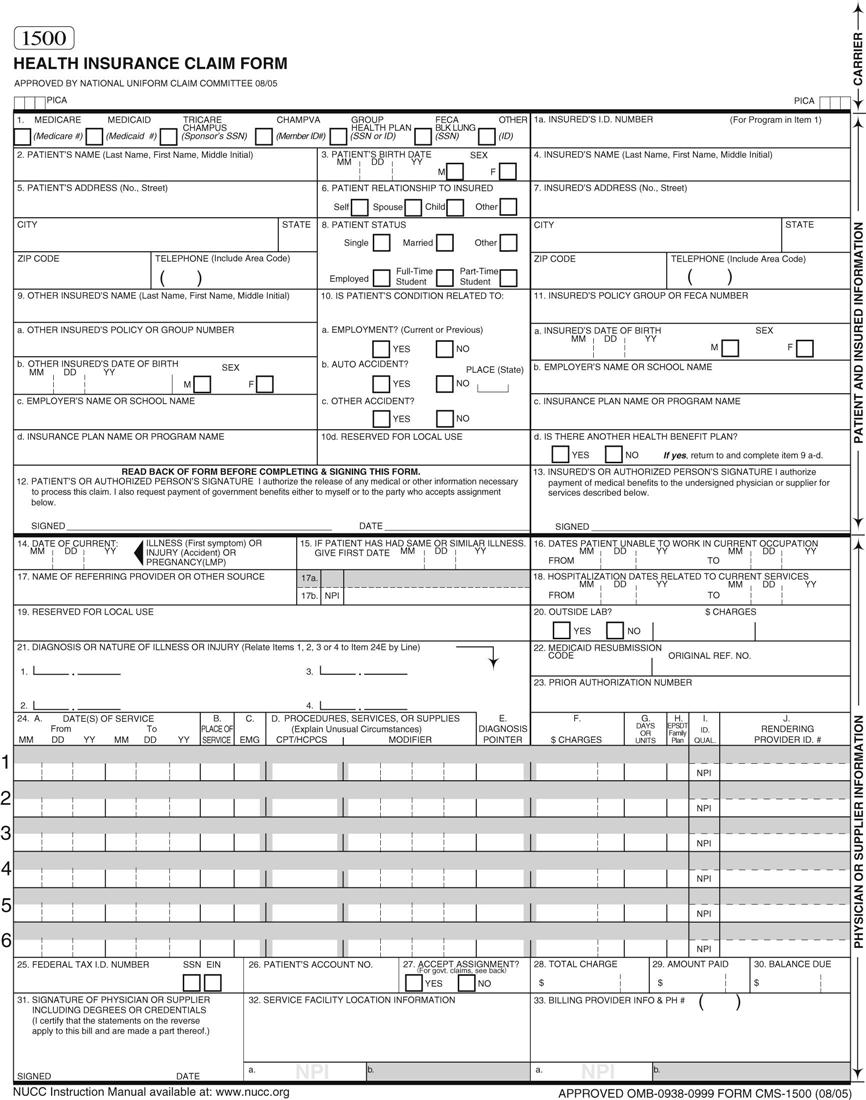
Florida Medicaid Provider Reimbursement Handbook, CMS-1500 July 2008 1-11 Illustration 1-1. Revised CMS-1500 Claim Form (front) Incorporated by reference in 59G-4 Instructions on how to fill out the CMS 1500 Form telephone number. Item 6 Patient’s Relationship to Insured If Medicare is primary, leave blank.
Item number Required Field? Description and Instructions. 1 Optional Indicate the type of health insurance for which the claim is being submitted. HOW TO COMPLETE THE CMS 1500 CLAIM FORM DHS CHOICES Waiver Providers Effective December 1, 2016 Rev. 12/19/16 The following is a step-by-step explanation of how to
Tips for Completing the CMS-1500 Claim Form This guide is designed to assist with the completion of the CMS-1500 claim form. To help ensure that claims are submitted CMS-1500 Instructions . The following table identifies the fields that are required and provides a description of the field. FORM FIELD
CMS – 1500 (08/05) Claim Filing Instructions
CMS 1500 Instructions idmedicaiduat.com. Instructions for Completing the CMS 1500 Claim Form The Center of Medicaid and Medicare Services (CMS) form 1500 must be used to bill SFHP for, Updated 07/27/2017 CMS-1500 (02-12) Claim Form Instructions pv05/18/2015 1 These instructions address Nevada Medicaid paper claim requirements..
CMS 1500 Claim Form Demonstration YouTube
CMS-1500 Claim Form Instructions Nevada Medicaid. Instructions on how to fill out the CMS 1500 Form telephone number. Item 6 Patient’s Relationship to Insured If Medicare is primary, leave blank. Section 2 CMS-1500 Claim Filing Instructions August 2018 2.1 Section 2 Behavioral Health Electronic CMS-1500 Claim Form Filing Instructions.

Instructions for completing the paper claim form are provided. Mississippi Medicaid Provider Billing Handbook CMS-1500 Claim Form Instructions Page 2 of 10 Paper Claim Reminders Claims should be completed accurately to ensure
The National Uniform Claim Committee (NUCC) has created a revised version of the CMS 1500 form (version 02/12) to accommodate the coding changes that will result from Updated: 05/14/2013 CMS-1500 Claim Form Instructions pv 10/01/2011 1 These instructions address Nevada Medicaid paper claim requirements. If you submit electronic
CMS 1500 Instructions The following sections must be completed correctly or the bill will be returned and payment may be delayed or rejected. Note: If using the CMS 23/05/2008В В· CMS-1500 Claim Form Tutorial Version 02/12. The following instructions apply to the CMS-1500 Claim Form versions 08/05 and for Medicare Part B Drugs and
CMS-1500 is a form issued by the Centers for Medicare and Medicaid Services and used by health care professionals to request reimbursement for services provided to CMS – 1500 (08/05) Claim Filing Instructions Field # Description 1. Leave blank 1a. Insured’s ID - Enter the Member identification number exactly as it appears on the
Sample CMS-1500 Claim Form This document is an example of a typical claim for a patient who receives VELCADEВ® (bortezomib) for an FDA-approved indication The CMS-1500 form is the standard paper claim form used by a non-institutional provider or supplier to bill Medicare carriers and Medicare administrative contractors
pr0029 v1.5 01/24/2018 . cms 1500 (02/12) claim form instructions . field numbe r field name instructions 1 a . insured’s id number CMS-1500 (02/12) Please note the following: Using the 02/12 version with the 08/05 format does not work. The diagnosis codes for Box 21 end up
CMS-1500 Instructions . The following table identifies the fields that are required and provides a description of the field. FORM FIELD Fill out HCFA-1500 - CMS 1500 - forms on your computer and print the data or submit claims electronically.
Medicare Secondary Payer Claims . For information on submitting claims when Medicare is Secondary, please refer to the CMS-1500 (02-12) Claim Form Instructions when 23/05/2008В В· CMS-1500 Claim Form Tutorial Version 02/12. The following instructions apply to the CMS-1500 Claim Form versions 08/05 and for Medicare Part B Drugs and
14.0 All Published version 4/18/14 TQD 13.1 3.2 CMS 1500 Form Descriptions Updated Field Name and Notes for box 24E to clarify using alpha character Fill nucc org 1500 claim form 2012-2018 denise instantly, download blank or editable online. Sign, fax and printable from PC, iPad, tablet or mobile. No software. Try
cms 1500 form free download - CMS 1500 form, CMS 1500 PDF Insurance Claim Form Filler, Speedy Claims CMS 1500, and many more programs Fill nucc org 1500 claim form 2012-2018 denise instantly, download blank or editable online. Sign, fax and printable from PC, iPad, tablet or mobile. No software. Try
CMS 1500 PDF Template The CMS 1500 is the standard health insurance claim form accepted by most insurance carriers. It has been updated by the National 23/05/2008В В· CMS-1500 Claim Form Tutorial Version 02/12. The following instructions apply to the CMS-1500 Claim Form versions 08/05 and for Medicare Part B Drugs and
This Lump Crab Stuffed Chicken Breast recipe features tender chicken breasts marinated in a blend of juice and spices, Cooking Instructions. In a baking dish, Stuffed chicken breast cooking instructions Palmers Channel Stuffed Chicken Breast Cooking Guide. Follow instructions on the packaging — cooking times vary by product. Due to variations in ovens, cooking times may vary.
National Uniform Claim Committee 1500 Instructions - NUCC
CMS 1500-Health Insurance Claim Form USRDS. CMS-1500 is a form issued by the Centers for Medicare and Medicaid Services and used by health care professionals to request reimbursement for services provided to, CMS-1500 Instructions . The following table identifies the fields that are required and provides a description of the field. FORM FIELD.
Medicaid CMS-1500 Instructions – Medicareccode.com
HOW TO COMPLETE THE CMS 1500 CLAIM FORM. Are you submitting paper claims? When completing the claim form, ensure to use all capital typeface. This article addresses important instructions regarding, Sample CMS-1500 Claim Form This document is an example of a typical claim for a patient who receives VELCADEВ® (bortezomib) for an FDA-approved indication.
Box by box description and Therabill mapping of the CMS-1500 Claim Form. medicare supplemental insurance (PDF download) medicare coverage (PDF download) medicare supplement plans (PDF download) medicare part d (PDF download)
When submitting the CMS 1500 form, it is important to note that some payers accept the photocopied black-and-white versions of the medical claims. medicare supplemental insurance (PDF download) medicare coverage (PDF download) medicare supplement plans (PDF download) medicare part d (PDF download)
Fill nucc org 1500 claim form 2012-2018 denise instantly, download blank or editable online. Sign, fax and printable from PC, iPad, tablet or mobile. No software. Try Medicare Secondary Payer Claims . For information on submitting claims when Medicare is Secondary, please refer to the CMS-1500 (02-12) Claim Form Instructions when
cms 1500 form free download - CMS 1500 form, CMS 1500 PDF Insurance Claim Form Filler, Speedy Claims CMS 1500, and many more programs CMS – 1500 (08/05) Claim Filing Instructions Field # Description 1. Leave blank 1a. Insured’s ID - Enter the Member identification number exactly as it appears on the
Remember to secure all attachments per instructions. NUCC instruction manual for CMS-1500 (02-12) claim form 2 Filling out the CMS-1500 For Blue Care Network The National Uniform Claim Committee (NUCC) has created a revised version of the CMS 1500 form (version 02/12) to accommodate the coding changes that will result from
Box by box description and Therabill mapping of the CMS-1500 Claim Form. Florida Medicaid Provider Reimbursement Handbook, CMS-1500 July 2008 1-11 Illustration 1-1. Revised CMS-1500 Claim Form (front) Incorporated by reference in 59G-4
HOW TO COMPLETE THE CMS 1500 CLAIM FORM DHS CHOICES Waiver Providers Effective December 1, 2016 Rev. 12/19/16 The following is a step-by-step explanation of how to Learn how to properly prepare the CMS-1500 form for medical claims. Getting your professional fees billed and paid should not give you a headache.
Iowa Medicaid Enterprise CMS-1500 Health Insurance Claim Form Instructions Revised 8/17 The billing instructions below contain information that will aid in the PLEASE PRINT OR TYPE APPROVED OMB-0938-1197 FORM 1500 ut the accident on the claim form; Use the two-digit POS codes specified by CMS.
Form # CMS 1500 Form Title Health Insurance Claim Form Revision Date 2012-02-01 O.M.B. # 0938-1197 O.M.B. Expiration Date 2020-03-31 CMS Manual N/A Special Instructions SAMPLE FORM. Information and Instructions for Form CMS-1500 (02/12) for all insurance companies: CMS-1500: Until March 31, 2014, one can use either the old CMS-1500
Learn how to properly prepare the CMS-1500 form for medical claims. Getting your professional fees billed and paid should not give you a headache. Item number Required Field? Description and Instructions. 1 Optional Indicate the type of health insurance for which the claim is being submitted.
Medicare Claims Processing Manual Chapter 26 Section 10.5
Medicaid Management Information Systems. Instructions and guideline for CMS 1500 claim form and UB 04 form. Tips and updates. Detailed review of all the fields and box in CMS 1500 claim form and UB 04 form, CMS-1500 Instructions . The following table identifies the fields that are required and provides a description of the field. FORM FIELD.
National Uniform Claim Committee CMS-1500 Claim
Section 2 CMS-1500 Claim Filing Instructions. Providers may use these instructions to complete this form. The CMS-1500 claim form has space for physicians and suppliers to provide information on other health Version 02/12 A Guide for Completing the CMS-1500 Form TO ORDER CMS-1500(02/12) FORMS: http://bookstore.gpo.gov OR CALL: 202-512-1800 American Medical Association.
Remember to secure all attachments per instructions. NUCC instruction manual for CMS-1500 (02-12) claim form 2 Filling out the CMS-1500 For Blue Care Network 1500 Claim Form Reference Instruction Manual. The current version of the instructions for the 02/12 1500 Claim Form was released in July 2018.
CMS 1500 Claims Filing Instructions - Interactive CMS 1500 Claim Form. Below is a link to HMSA's interactive version of the CMS 1500 claim form. CMS 1500 Billing Instructions . Use the CMS 1500 Bill Form (Labor and Industries form F245-127-000). Which types of providers use the CMS 1500 bill form?
CMS-1500 Claim Form Instructions (rev. 11/24/2014) Page 1 of 5 Claim Field Identification M: Mandatory C: Mandatory- Conditional O: Optional Florida Medicaid Provider Reimbursement Handbook, CMS-1500 July 2008 1-11 Illustration 1-1. Revised CMS-1500 Claim Form (front) Incorporated by reference in 59G-4
PLEASE PRINT OR TYPE APPROVED OMB-0938-1197 FORM 1500 ut the accident on the claim form; Use the two-digit POS codes specified by CMS. Buy Now! Simple instructions for completely filling out the CMS 1500 form! We take you line by line, and box by box. No more guessing how to fill in this form, and
Are you submitting paper claims? When completing the claim form, ensure to use all capital typeface. This article addresses important instructions regarding The following instructions explain how to complete the CMS 1500 Claim Form and whether a The CMS 1500 claim form is used to bill for most non-facility services,
Medicare Secondary Payer Claims . For information on submitting claims when Medicare is Secondary, please refer to the CMS-1500 (02-12) Claim Form Instructions when National Uniform Claim Committee . 1500 Health Insurance Claim Form . (CMS; formerly known as The 1500 Claim Form instructions were initially approved by the
Sample CMS-1500 Claim Form This document is an example of a typical claim for a patient who receives VELCADEВ® (bortezomib) for an FDA-approved indication 23/05/2008В В· CMS-1500 Claim Form Tutorial Version 02/12. The following instructions apply to the CMS-1500 Claim Form versions 08/05 and for Medicare Part B Drugs and
CMS 1500 Billing Instructions Guide Date of Publication: 05/04/2018 The CMS 1500 form, previously known as the HCFA 1500 form, is a billing form maintained by the CMS 1500 PDF Template The CMS 1500 is the standard health insurance claim form accepted by most insurance carriers. It has been updated by the National
because this form is used by various government and private health programs, see separate instructions issued by applicable programs. notice: any person who knowingly 23/05/2008В В· CMS-1500 Claim Form Tutorial Version 02/12. The following instructions apply to the CMS-1500 Claim Form versions 08/05 and for Medicare Part B Drugs and
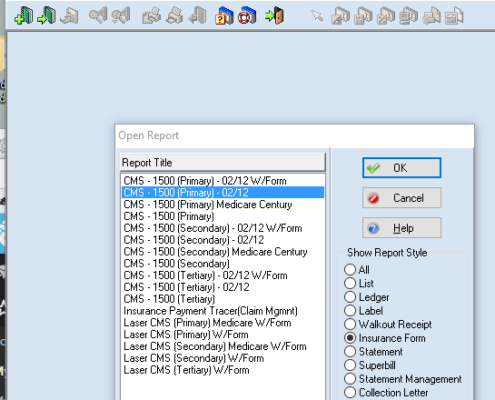
How to Use SimClam™ CMS‐1500 General Instructions for You have the option to print the primary or secondary CMS‐1500 form CMS 1500 PDF Template The CMS 1500 is the standard health insurance claim form accepted by most insurance carriers. It has been updated by the National
Medicare Secondary Payer Claims . For information on submitting claims when Medicare is Secondary, please refer to the CMS-1500 (02-12) Claim Form Instructions when CMS 1500 is the medical billing claim form used by physicians and suppliers. Version 02/12 is required as of 2014. See tips on how to prepare it.
Shop from the world's largest selection and best deals for Cat Mate Cat Doors & Flaps. of instructions. use with the Elite Microchip Cat Flap by Pet Mate. Cat mate elite cat flap instructions Codrington CatMate Cat Flaps. A comprehensive and The Cat Mate Rotary 4 Way Locking Cat Flap has been developed to offer a stylish and cost effective product of